The annotated images in this case discussion are all scrollable panels. To use the panels, hover your cursor over the panels (on mobile, tap the panel once) and then unlock them by clicking the lock icon. Now you can scroll with your mouse and use any of the viewing tools.
Click the colored links in the discussion text to make the designated panel show the relevant finding.
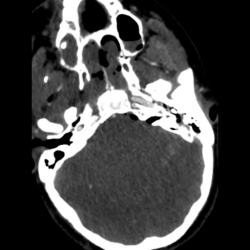
This is a busy case with many findings. I always start with the brain and intracranial findings before getting bogged down on all the fractures. There are multifocal areas of parenchymal hemorrhage (red arrows) with hemorrhages in the left frontal lobe inferiorly annotated on the above panel. Additional multifocal subarachnoid hemorrhages are also present (blue arrows) shown in particular in the medial left middle cranial fossa, the left sylvian fissure, the left frontal lobe, and the left upper cervical spine. Finally, there is subdural blood and gas in the left temporo-occipital junction convexity (green arrow).
Additional findings are the presence of subarachnoid gas in the basilar cisterns as well as diffuse effacement of the sulci and particularly the basilar cisterns suspicious for cerebral edema. Now on to the fractures!
Knowing the basic fracture patterns can be helpful in cases like this, more than anything to know what fractures tend to occur together and to be more concise in our impressions.
The components of a naso-orbito-ethmoid (NOE) fracture pattern are present including fracture of the nasal bone (right sided, shown on axial), medial orbital walls, adjacent ethmoid sinuses (the exact fractures are difficult to see but the substantial opacification implies fractures), and the nasal septum (seen best on the coronal plane, both anteriorly and posteriorly).
On the left, there are fractures of the pterygoid plates (red arrow on axials). Whenever, you see pterygoid plate fractures, look for the other component of LeFort fracture patterns. On the coronal images, a horizontal fracture of the left anterolateral nasal aperture with associated horizontal fracture of the left lateral maxillary sinus wall are present completing a LeFort I pattern (red arrows).
There is fracture of the anteromedial orbital wall, the inferior orbital rim and floor, which combined with the nasal bone and lateral maxillary sinus wall fractures form the components of a LeFort II pattern. However, I do not think that the nasal bone fracture has the characteristic transverse orientation you’re supposed to have for a LeFort II and it seems separate and not extending to the medial orbital wall fracture. Therefore, I would just describe the components here and not specifically mention that there is a LeFort II fracture (this study was however read as having a LeFort II fracture so not everyone always agrees).
There is no lateral orbital rim or zygomatic arch fractures on the left so no LeFort III. No pterygoid plate fracture on the right means no LeFort fracture on that side.
The components of a ZMC fracture are present on the right: fracture of the zygomatic arch and mild diasthasis at the zygomatico-temporal suture (red arrows – axial), comminuted fracture of the antero-medial maxillary sinus walls near the zygomatico-maxillary suture (blue arrows – axial), fracture of the zygomatico-sphenoid suture (green arrows – axial), and fracture at the level of the zygomatico-frontal suture (red arrow – coronal).
Once I’ve done a pattern based search for the fractures, I then go through the paranasal sinuses, nasal cavity, orbits, and skull base and see what’s fractured.
In the paranasal sinuses, there is fracture of the right frontal sinus inner wall with intracranial extension (red arrow). All the walls of the sphenoid sinuses and the sphenoid septum have been fractured (blue arrows). A fracture fragment protrudes to the right superior orbital fissure (rightmost blue arrow).
When looking at the sphenoid and ethmoid sinuses, it’s important to look at the roofs, best seen on coronal and sagittal planes. Here, the ethmoid roof and the planum sphenoidale are fractured, predisposing the patient to CSF leakage.
All the walls of the maxillary sinuses are fractured (green arrows), some of which we have already discussed as part of the fracture patterns.
In the orbits, on the right, all the walls are fractured (panel A – red arrows), including the roof with intracranial extension and pneumocephalus. The orbital floor fracture is comminuted and highly depressed. On soft tissue recons, there is herniation of orbital fat and inferior rectus muscle through the fracture defect (panel B – blue arrow). The inferior rectus muscle is thickened compared to the contralateral side consistent with intramuscular hematoma. Clinical assessment for the presence of entrapment is likely prudent. Also mention how much orbital hemorrhage there is, here mainly extra-conal and in the supero-lateral orbit (panel B – green arrow).
On the left, there is also a fracture of the roof. The medial and floor fractures we have already described. There is not much displacement of the fractures and not as much intra-orbital hemorrhage.
The globes should be assessed and here there is no evidence of injury. There is of course peri-orbital soft tissue swelling and gas.
Finally, looking at the remaining skull base/calvarium, one sees that the right sphenoid sinus fractures have a component extending along the greater wing of the right sphenoid (red arrow).
In the nasal cavity, there is a fracture of the right hard palate (blue arrow). This and palate fractures in general are also very well seen on coronal reformations.
Interrogating the mastoids and middle ears, there is most likely a left mastoid fracture given the large effusion in the mastoids and middle ear (green arrow). However, the fracture line is not evident on these images.
No Comments yet!